
- Learning outcomes
- Definitions
- Venous thromboembolism (VTE)
- Pulmonary thromboembolism (PE)
- Systemic (arterial) thromboembolism
- Paradoxical embolism
- Non-thrombotic embolism
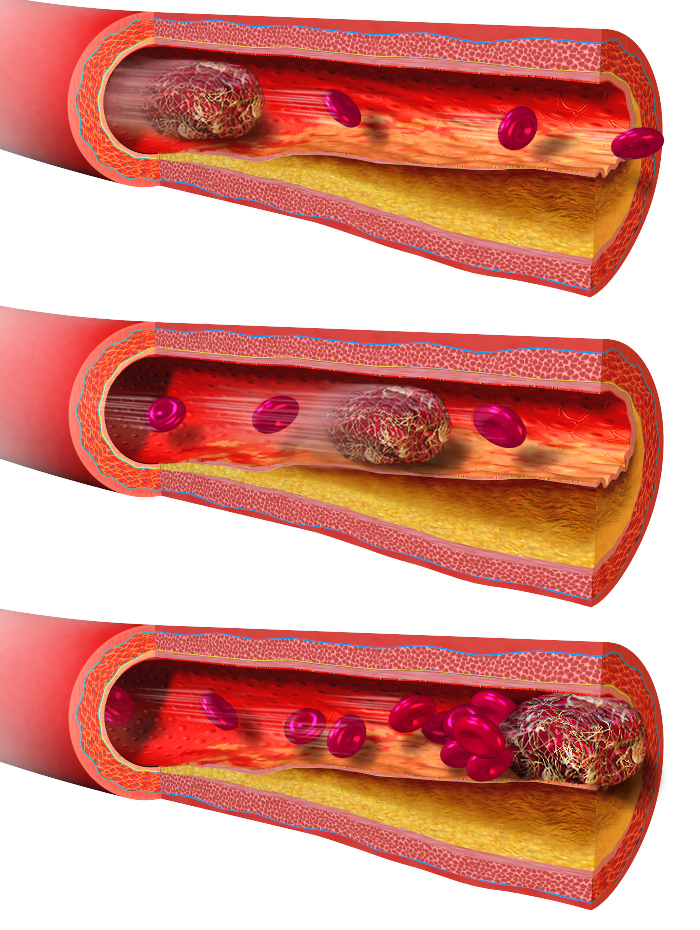
Blood vessels are designed to carry blood in a liquid state. However, as we have learnt in an earlier blog, blood can be abnormally converted to a solid-or semi solid mass, which is termed as a thrombus. The thrombus may remain at the site of formation, or it may detach and become a thromboembolus.
The transference of any abnormal material by the blood stream and its subsequent impaction in a distal blood vessel is known as embolism. Thromboemboli are the most common form of emboli, but other materials such as fat, air, amniotic fluid and foreign bodies may also embolise. In this blog, we will learn about the pathophysiology and the clinical consequences of embolisation, with particular emphasis on venous and arterial thromboembolism.
Learning outcomes
- Elaborate what is meant by embolism and thromboembolism
- Describe the cause, pathophysiology and complications of venous (VTE) and pulmonary thromboembolism (PE)
- Contrast the clinical consequences and complications of arterial thromboembolism as compared to venous thromboembolism
- Distinguish infarct from ischaemia and its clinical consequences
- Describe the pathophysiology and clinical features of other forms of embolism apart from thromboembolism
Blausen.com staff (2014). “Medical gallery of Blausen Medical 2014“. WikiJournal of Medicine1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. – Own work
Definitions
The word embolus derives from the greek work en-ballein, meaning ‘to throw’. Embolism is therefore the pathological condition, where an abnormal material (which could be a thrombus, gaseous material, fat or foreign material) is transferred by the blood stream from one point to another point where it becomes lodged or impacted.
Thromboembolism refers specifically to the condition where a thrombus or part of thrombus is transferred from its site of origin to another site distal to where it first formed.
The movement follows the blood stream and the thromboembolus impacts at the narrowest point relative to the size of the embolus. Therefore, it follows that venous thromboemboli impact in the pulmonary vasculature after it has moved through the large veins and right cardiac chambers. Arterial thromboemboli though will impact in the smaller branches of the arteries.

Venous thromboembolism (VTE)
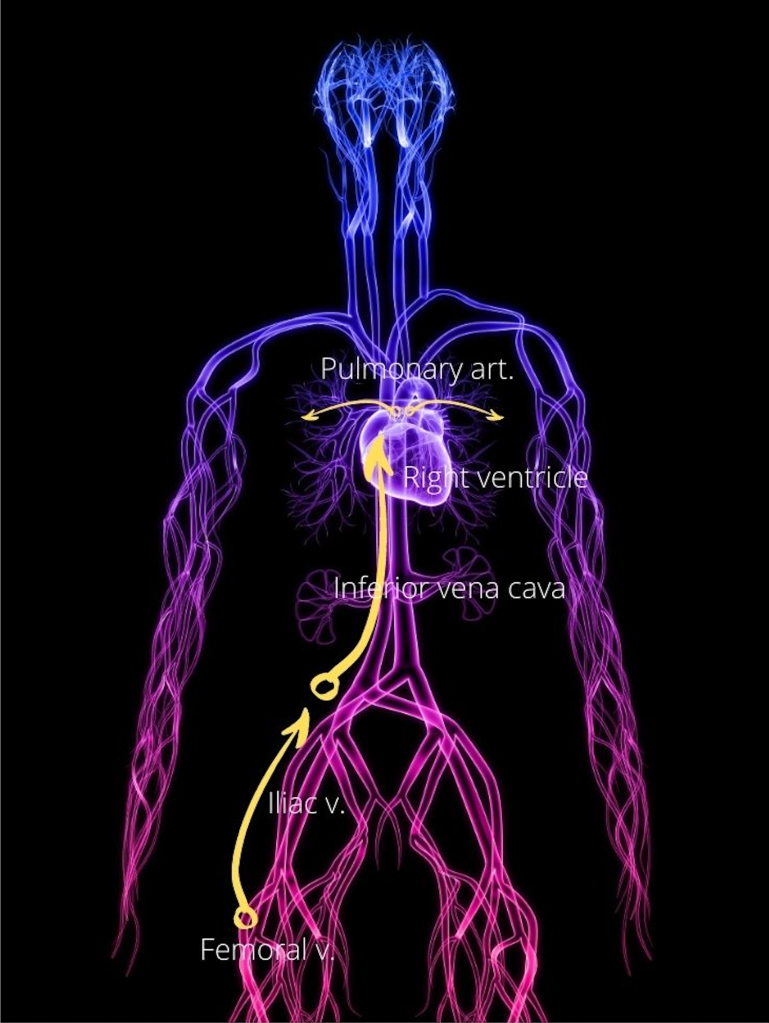
The most common source for VTE is from the deep veins of the leg. As explained in the earlier blog, thrombosis involving the leg veins is known as deep vein thrombosis (DVT).
Venous thrombi can also arise from other sites such as the subclavian vein, usually secondary to malignancy, trauma and central venous line placement. Rarely, venous sinus thrombosis of the brain may be seen in patients with hypercoagulable state and vaccine induced thrombotic thrombocytopenia.
Whatever the source, the dislodged venous thrombi will move through the large bore inferior or superior vena cava, and then pass through the capacious right atrium and ventricle into the pulmonary artery. Here the calibre of the arteries begin narrowing. Depending on the size of the emboli, it may therefore become impacted in the pulmonary trunk if large, or move distally to impact in the smaller branches of the pulmonary artery. Venous emboli that becomes trapped in the pulmonary artery and its branches is called pulmonary thromboembolism (PE).
Pulmonary thromboembolism (PE)
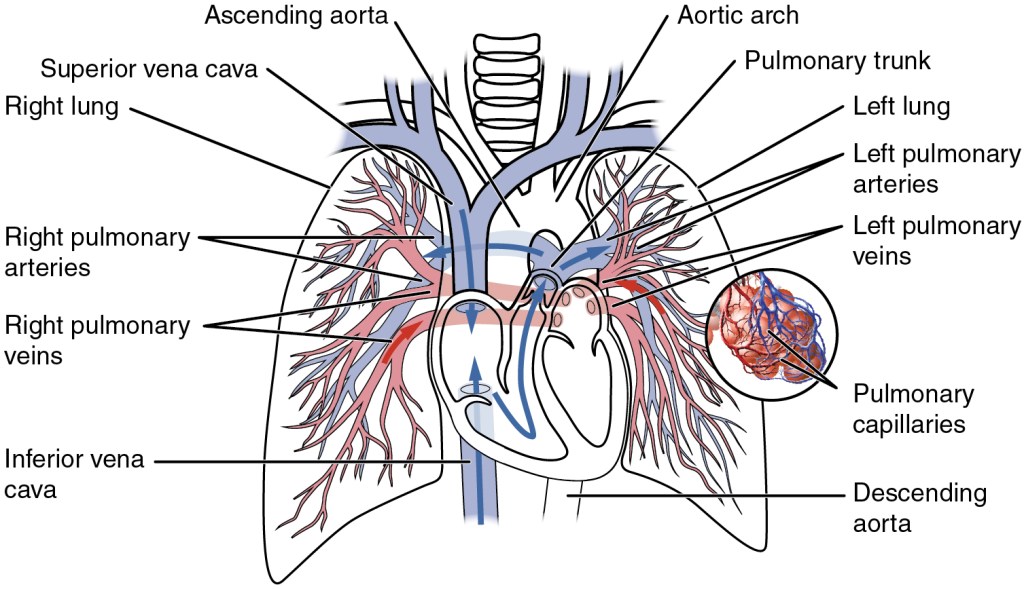
Illustration from Anatomy & Physiology, Connexions Web site. http://cnx.org/content/col11496/1.6/, Jun 19, 2013
The clinical consequences and outcome of PE would depend on
- The location in the pulmonary artery where the embolus lodges. Large emboli would lodge in the pulmonary trunk or main branches of the pulmonary artery, while smaller emboli may move distally to the smaller branches of the pulmonary artery.
- Number of emboli. A shower of emboli may block several arteries within a short time.
- Proportion and rate of pulmonary arteries occluded.
- Underlying cardio-respiratory status of the patient.
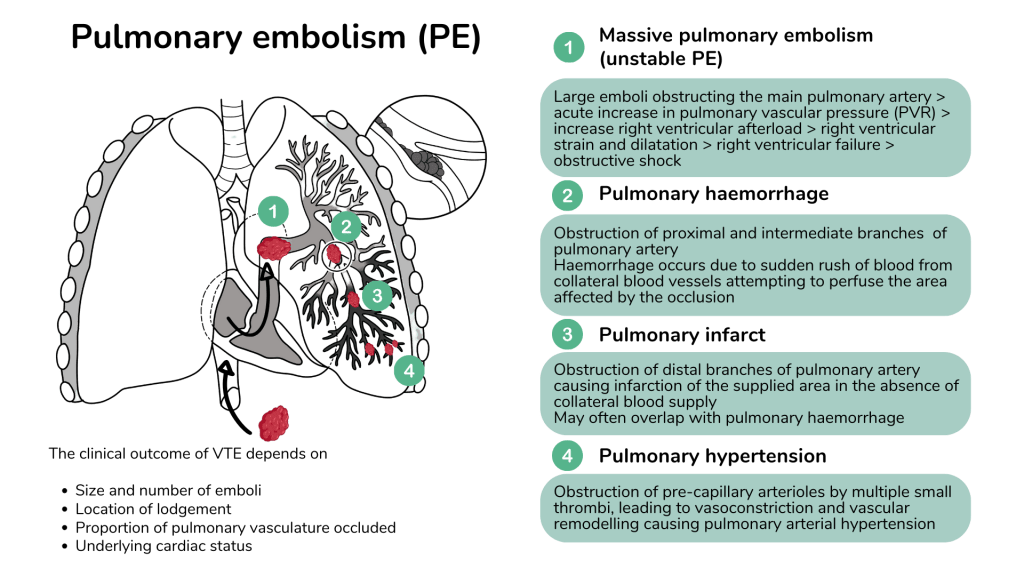
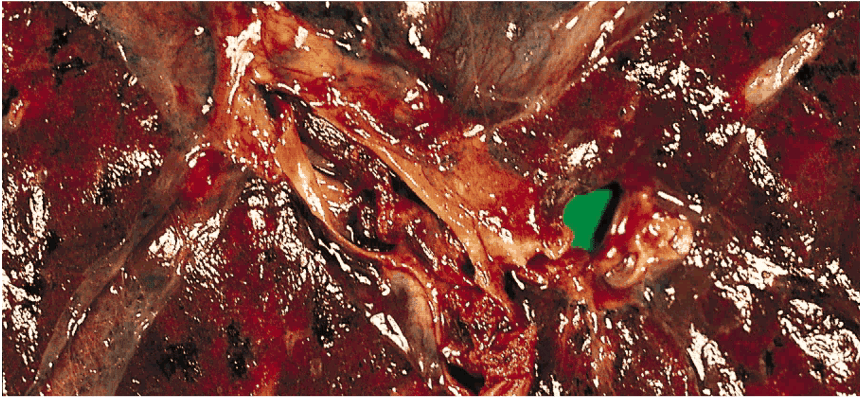
Massive pulmonary embolism
Massive pulmonary embolism occurs in about 5% of PE. This condition results from a large embolus that lodges in the main pulmonary trunk (saddle thrombus) and occludes more than 60% of the pulmonary artery blood flow.
The sudden disruption in blood flow and increase in back pressure and strain on the right ventricle causes acute right heart failure and may lead to sudden death unless immediate intervention is taken.
Video showing a pulmonary embolectomy in a woman with deep vein thrombosis and saddle pulmonary embolism. Please click to watch on YouTube.
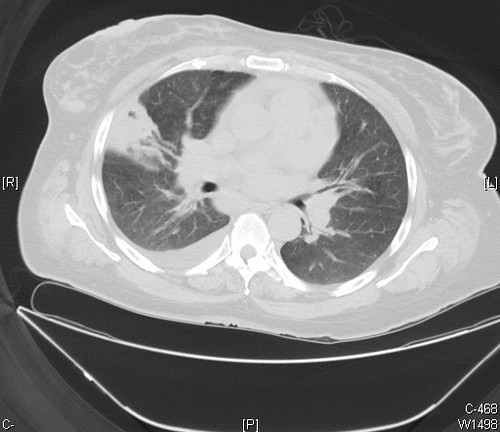
- The infarct in this Ct scan is represented by the wedge shaped density in the right lung with its base abutting the pleura. (“Pulmonary infarction, right lung Case 209” by Pulmonary Pathology is licensed under CC BY-SA 2.0)
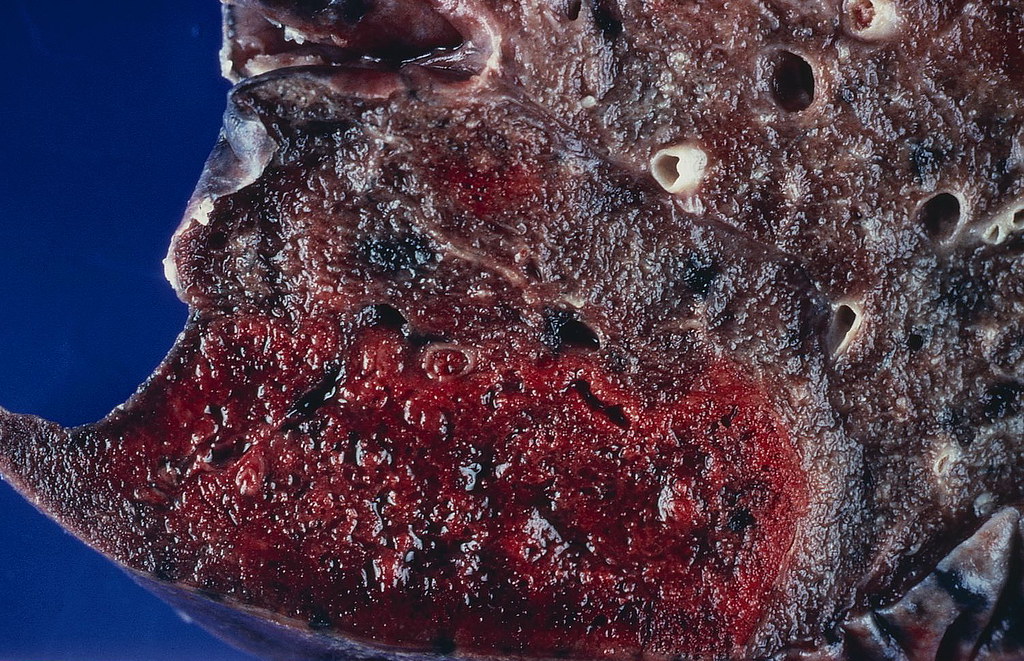
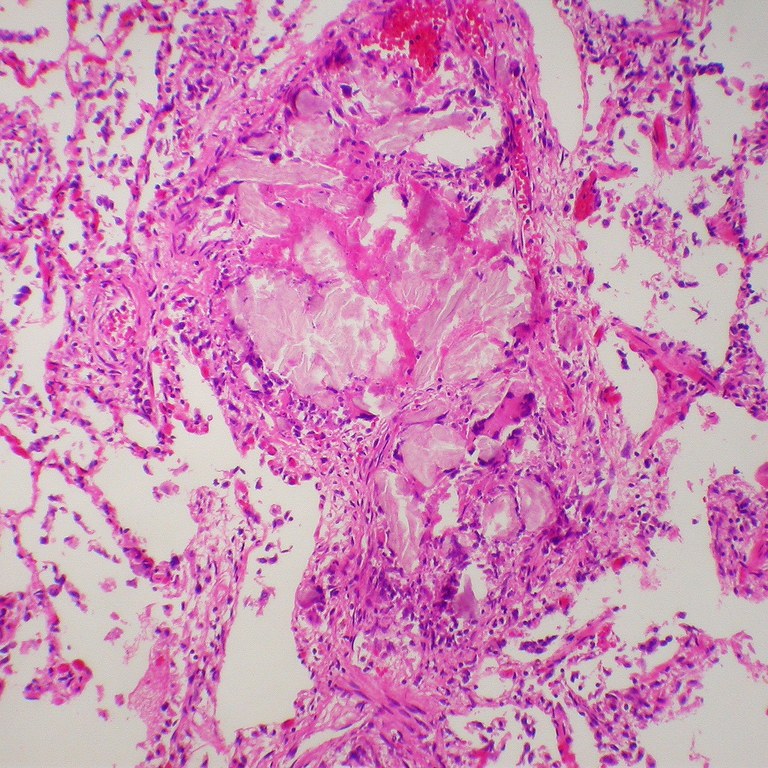
- Recent haemorrhagic infarct of the lung. (“Recent hemorrhagic infarct” by Pulmonary Pathology is licensed under CC BY-SA 2.0)
Systemic (arterial) thromboembolism
Systemic embolism refers to an embolus that occurs in the arterial circulation. The most common origin of the thrombus is from the heart and accounts for about 80% or arterial emboli. Other sites of thrombus origin include the aorta, neck veins (carotid artery) and intracranial arteries.
As discussed in the previous blog on thrombosis, thrombus in heart is usually caused by atrial fibrillation, valvular heart disease and myocardial infarction as a result of stasis and turbulent blood flow. Infective and non-bacterial endocarditis can also cause embolisation of cardiac vegetations.
Atherosclerosis and ruptured plaques also contribute to thrombus formation in the arteries that embolise to various organs particularly in the heart and brain, causing myocardial infarction and stroke respectively.
Systemic emboli travel through the blood stream and lodge in the smaller branches of arteries. The sudden occlusion of the artery and disruption of blood flow can cause ischaemia or infarction of the area supplied. For example, in a stroke, the emboli may travel from a detached mural thrombus in the cardiac chamber, or a thrombus from an atherosclerotic plaque in the carotid artery, to the cerebral artery causing cerebral infarction.

Paradoxical embolism
As described earlier, venous thromboembolism (VTE) terminates in the pulmonary artery causing the various manifestations of pulmonary embolism (PE) while systemic thromboembolism terminates in the arteries of systemic organs causing ischaemia and infarction.
Strictly speaking, right sided venous emboli stay in the right and left sided systemic emboli stay on the left. However, in rare cases, a right sided venous emboli may enter into the left sided systemic circulation. This phenomenon is called paradoxical embolism and occurs in the presence of an abnormal intracardiac or pulmonary veno-arterial shunt. Congenital cardiac malformations such as patent foramen ovale, atrial septal defect and ventricular septal defect may create a passage for the venous embolus to bypass the lungs and move directly from the right cardiac to left cardiac chambers and thereafter into the systemic circulation.
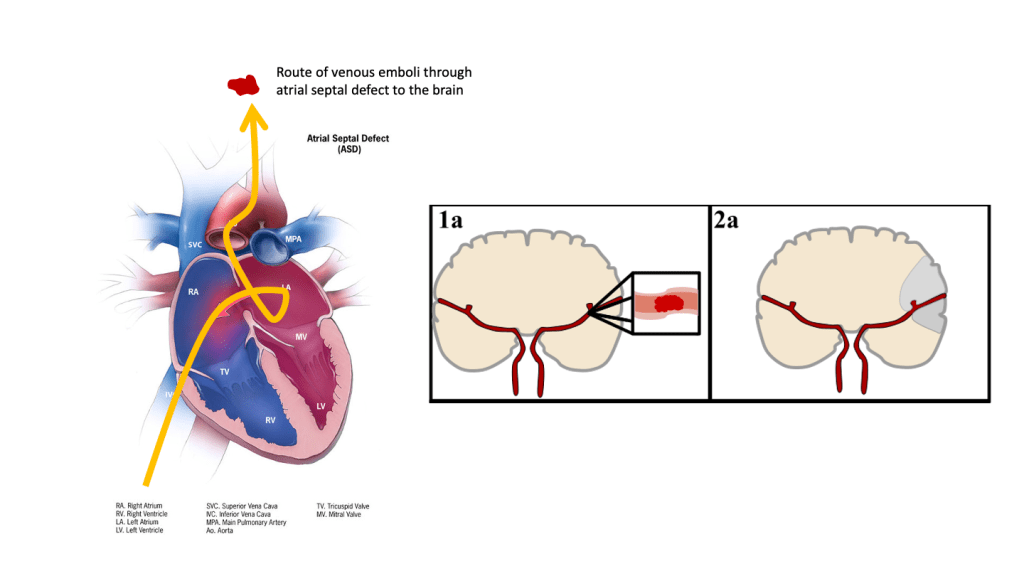
Figure modified from: ElinorHunt, CC BY-SA 4.0, via Wikimedia Commons
Non-thrombotic embolism
Fat embolism
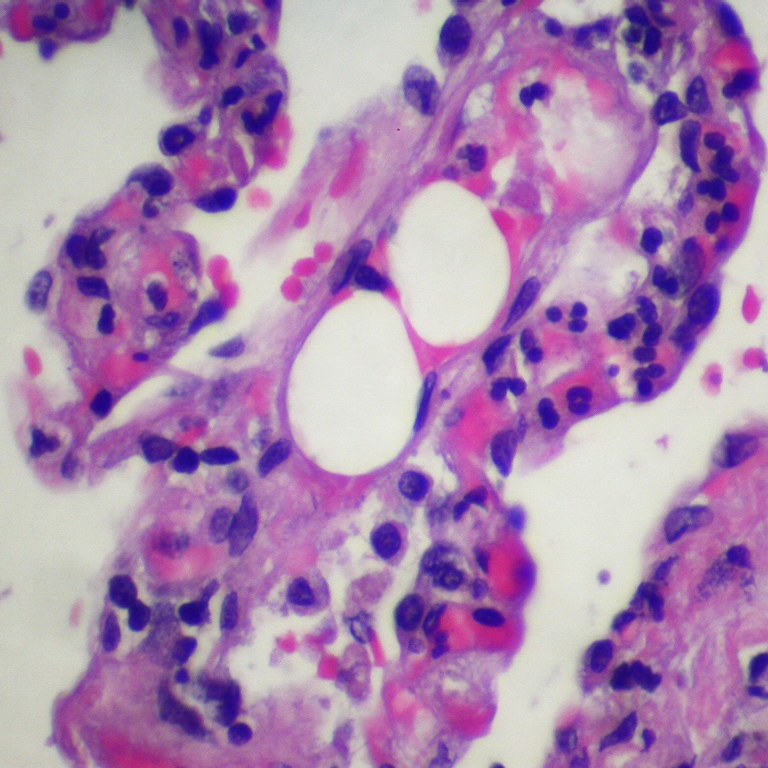
Fat globules may be introduced into the blood vessel from the fat spaces in bones when there is a fracture. Fat embolism may be seen in 5-10% of patients with pelvic or multiple long bone fracture. Other causes of fat emboli include surgical procedures such as liposuction and acute pancreatitis.
The fat emboli may enter the lung and cause acute hypoxia, into the brain causing neurological deficits and the skin causing petechiae.

Air embolism
Air embolism may result from trauma of the neck and chest with breach of the blood vessels, uterine contraction and air insufflations in abortions, laparoscopic procedures and during delivery. It is a recognised complication of deep sea diving and results in Caisson disease or decompression sickness.
Amniotic fluid embolism
Amniotic fluid embolism (AFE) is a rare complication of pregnancy, where amniotic fluid or foetal cells enter the maternal circulation. This often leads to cardiovascular collapse and haemorrhage from disseminated intravascular coagulation (DIC). AFE can be fatal. Risk factors include abdominal trauma, abortion, eclampsia and caesarean section.

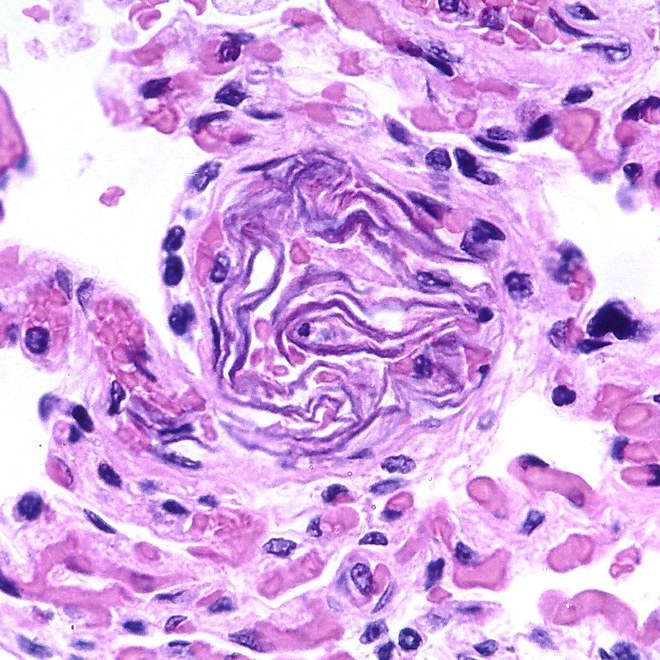
- “Amniotic fluid embolism” by Pulmonary Pathology is licensed under CC BY-SA 2.0
- “Fat embolism” by Pulmonary Pathology is licensed under CC BY-SA 2.0
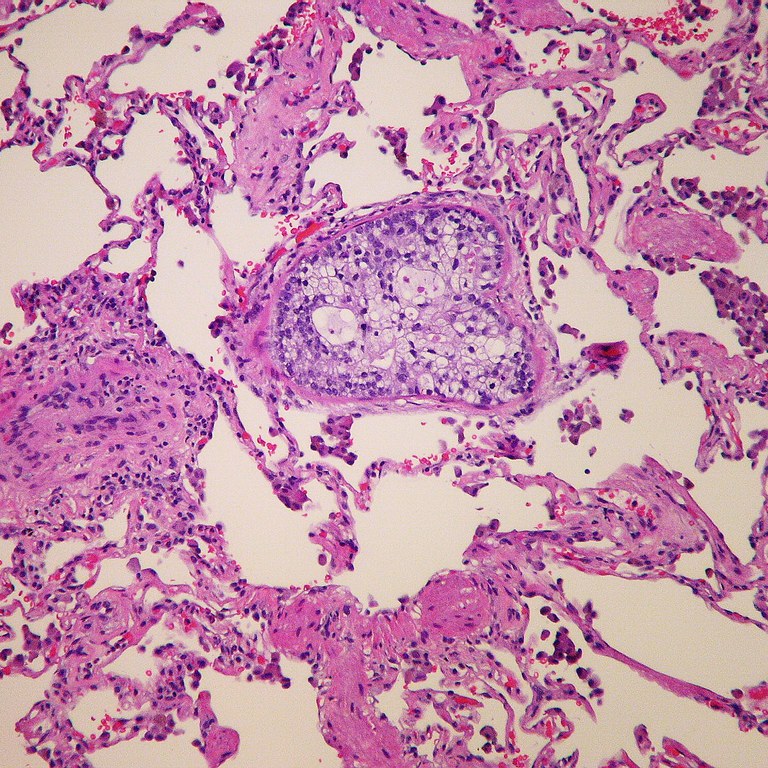
- “Microcrystalllne cellulose – Foreign body pulmonary embolization in an intravenous drug abuser” by Y. Rosen, MD is licensed under CC BY-SA 2.0
- “Tumor embolus” by Pulmonary Pathology is licensed under CC BY-SA 2.0

{kind=link}