Learning outcome
- Describe the pathogenesis, clinical and laboratory feature of immune thrombocytopenia purpura.
Pathophysiology
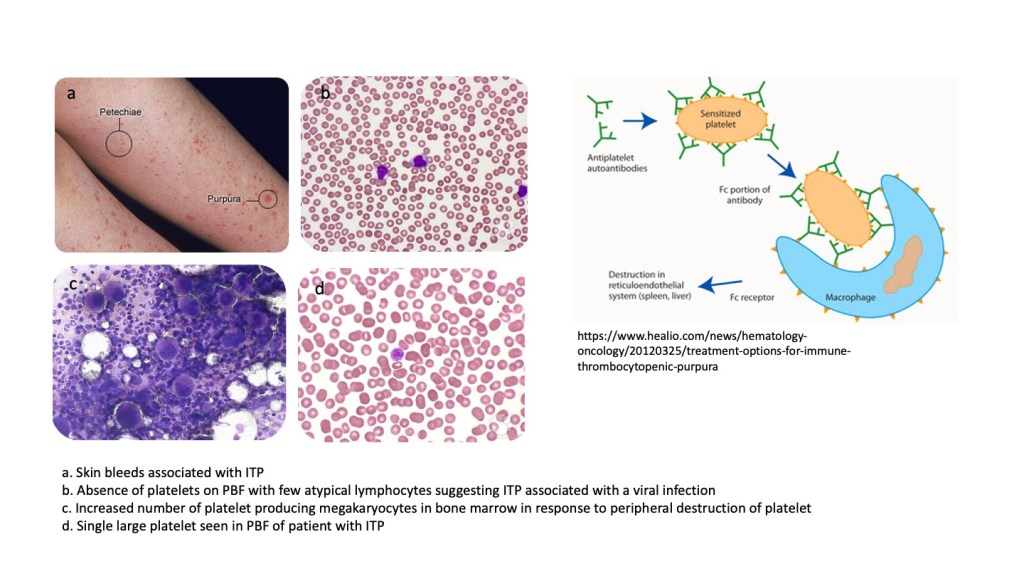
Immune thrombocytopenia purpura (ITP) is a condition characterised by low platelet counts resulting from immune destruction of platelets. Auto-antibodies to platelet antigens develop (similar to that seen with red cells in autoimmune haemolytic anaemia) and coat the patient’s platelets that are subsequently removed by the splenic macrophages that recognise the IgG sensitised opsonised platelets.
In order to keep up with the increased destruction of platelets in the spleen, megakaryocytes proliferate in the marrow to increase the output of platelets into the bloodstream.
Clinical features
Immune thrombocytopenia purpura can occur at any age, but is more commonly seen among children and young adults. Among those aged above 12 years, females are more commonly effected.
Two clinical types of ITP are recognised:
- an acute self-limiting type, usually seen in children following an infection, that resolves spontaneously
- a chronic type that recurs over months to years
Patients usually present with skin or mucosal bleeding such as petechiae, purpura, ecchymoses, epistaxis and gum bleeding. More severe bleeds such as haematuria, hemetemesis, melaena and intracranial bleeds may be observed. Mild splenomegaly is noted in about 10% of patients, Typically, patients with ITP do not have hepatomegaly or lymphadenopathy.
Laboratory features
The full blood count and peripheral blood film is generally unremarkable except for the thrombocytopenia. Atypical lymphocytes may be present especially if the ITP is associated with a preceding infection. Occasional large platelets may be observed as young platelets are pushed into the circulation. Coagulation tests (APTT, PT) will be normal.
Bone marrow examination may be indicated, especially in older adults. The characteristic feature on the bone marrow is megakaryocytic hyperplasia as the marrow increases its platelet production capacity in an attempt to replace the platelets that are destroyed by the spleen.
Management
No treatment and ‘watchful waiting’ is recommended for mild cases and most cases of acute ITP in children.
The mainstay of treatment is immunosuppression with prednisolone to attenuate the immune destruction that occurs in the spleen. In steroid refractory cases, rituximab, a monoclonal antibody that attacks B-lymphocytes may be used. Splenectomy may be indicated in chronic cases not responsive to standard therapy with steroids and rituximab.
