Learning outcome
Distinguish the use of common laboratory tests (Platelet count, APTT, PT, TT) to assess abnormalities of the coagulation cascade
Clinical assessment and classification of bleeding disorders
The clinical assessment of a patient with suspected bleeding disorder should include evaluation of;
- Age of onset and gender
- Extent and type of bleeding – skin, mucosal, ocular, menorrhagia, gastrointestinal, visceral, intra-articular
- If bleeding was spontaneous or provoked e.g. following trauma, post-operative
- Family history of any bleeding
- Bleeding history – umbilical stump bleeding, bleeding following circumcision, tooth extraction
- Drugs – NSAIDS, anti-coagulants, antibiotics
- Alcohol consumption and liver disease
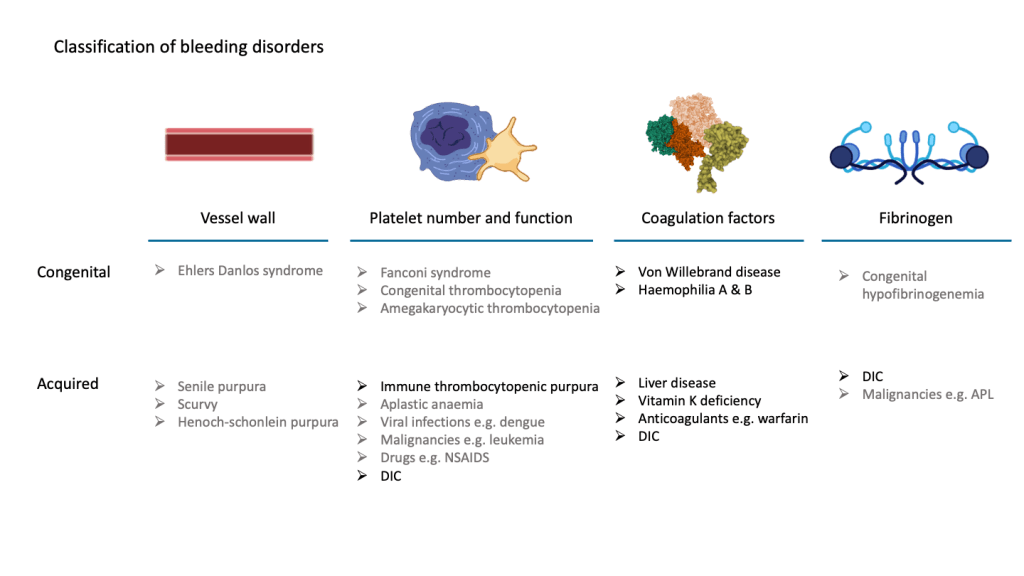
As described in the previous section, many components are responsible for maintaining haemostasis and disorders in each of the components may contribute to bleeding as illustrated below.
Laboratory investigation of bleeding disorders
A through bleeding history should always be obtained before proceeding to perform tests in a patient with suspecting bleeding disorder. Bleeding assessment tools (BAT) are helpful to quantify the patient’s subjective experience of bleeding and bruising.
Platelet count
The normal platelet count is 150 – 400 x 109/L. Thrombocytosis i.e. high platelet counts may occur with iron deficiency, following a haemorrhage or in myeloproliferative neoplasms.
A low platelet count is referred to as thrombocytopenia. Bleeding manifestations usually do not occur until platelet counts are below 100 x 109/L.

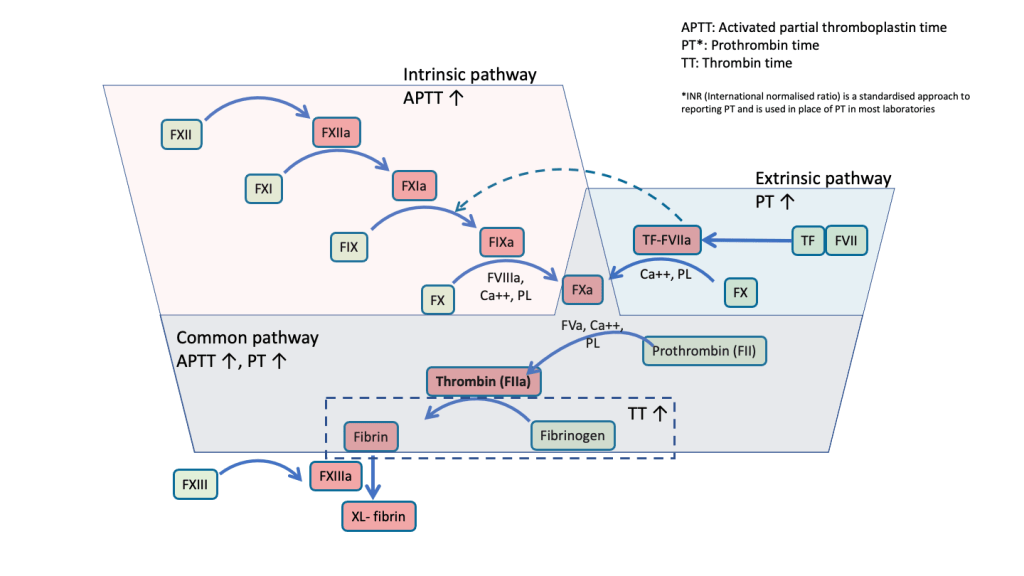
Activated partial thromboplastin time (APTT)
The APTT is a test that assesses the coagulation factors involved in the intrinsic and common pathways. An isolated prolongation of APTT without prolonged PT is usually indicative of a deficiency of either FVIII, FIX, FXI or FXII. Deficiency of vWF associated with von Willebrand disease also causes a prolongation of APTT. This is because vWF is a carrier molecule for FVIII and a deficiency of vWF will also cause low FVIII.
Prothrombin time (PT)
The PT assesses coagulation factors in the extrinsic and common pathways. Isolated prolongation of PT can occur due to FVII deficiency, either congenital, or acquired following therapy with anticoagulants such as warfarin. Prolongation of both PT and APTT is commonly seen in liver disease, vitamin K deficiency, anticoagulant therapy and DIC.
Thrombin time
TT is prolonged when there is either a deficiency or abnormality of fibrinogen. It is commonly seen with acquired hypofibrinogenemia following DIC and hyperfibrinolysis. Anticoagulants that interfere with thrombin activity such as heparin and dabigatran also cause prolongation of TT.
