Learning outcomes
- Explain the biochemistry of folate in relation to the pathogenesis of megaloblastic anaemia
- Describe the absorption and transport of folate
- List the causes of folate deficiency
Biochemistry of folate
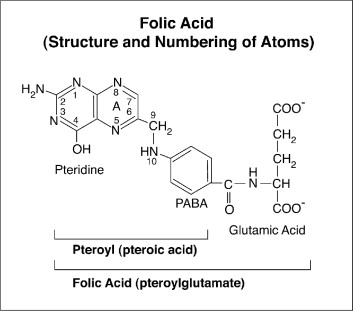
Folate is an essential water-soluble B vitamin, that consists of a molecule of para-aminobenzoic acid (PABA), with its amino end attached to a pteridine ring, and its carboxyl group attached to the α-amino group of glutamic acid (Glu).
The major role of this vitamin is to synthesize DNA by one-carbon transfers in the body.
Thymidylate synthase
Impaired methylation of deoxyuridylate (dUMP) to deoxythymidylate (dTMP) by thymidylate synthase in the formation of DNA leads to megaloblastic anaemia. In this step, N5,N10-methylene THF transfers its methyl group to dUMP, thereby generating dTMP which is utilised in DNA synthesis.
N5,N10-methylene THF is converted to N7,N8 dihydrofolate (DHF) in the process, which is then reduced by dihydrofolate reductase (DHFR) to THF. N5,N10-methylene THF can thus be regenerated from the produced THF by methyl transfer from serine by serine hydroxymethyl transfer, for synthesis of dTMP by thymidylate synthase.
Folate deficiency results in impaired dTMP generation that is required for incorporation into growing DNA strands, with accumulation of dUMP instead. This leads to mis-incorporation of dUMP instead of dTMP into DNA strands, which results in DNA strand breaks, fragmentation and apoptotic cell death. Cells also arrest in S phase and slows maturation.
Methionine synthase
In addition to this action, folate also has diverse roles in amino acid interconversions and methylation reactions. One of the most important folate-dependent teactions is the conversion of homocysteine to methionine in the synthesis of S-adenosyl-methionine, an important methyl donor. In this reaction catalysed by methionine synthase, N5-methyl THF acts as a methyl donor to homocysteine to generate methionine and THF. This reaction also requires vitamin B12 as a co-factor.
Deficiency of either folate or vitamin B12, therefore can result in reduced levels of methionine with accumulation of homocysteine.
Folate requirements
Folate is present naturally in many food types. Vegetables particularly dark green leafy vegetables, fruits, nuts, beans, peas, seafood, eggs, dairy products, meat, poultry, and grains are all good sources of folate. Spinach, liver and asparagus are among the foods with the highest folate levels (at least within a Western diet). Folate is however highly labile and is easily destroyed by cooking.
The recommended daily intake of folate is 400 ug, which should be sufficient to meet the daily demands of about 50 ug. However, daily intake may need to be increased in vulnerable populations that would have higher needs. This would include:
- Pregnant women require more folate because of its role in nucleic acid synthesis. Folate supplementation during pregnancy is recommended.
- Women of childbearing age should receive adequate folate to reduce the risk of neural tube defects and other birth defects, which have been associated with folate deficiency in foetal life.
- Patients with chronic haemolysis (e.g., thalassaemia), myeloproliferative disorders (e.g. polycythaemia vera) and conditions with rapid cell turnover (e.g. exfoliative dermatitis). Sufficient folate is required to maintain erythropoiesis in the setting of high rate of cell turnover in these patients.
- Alcoholics. Apart from their poor diet, alcohol interferes with folate absorption and hepatic uptake, accelerates folate breakdown, and increases its renal excretion.
- Patients with malabsorption disorders e.g. coeliac disease, tropical sprue, inflammatory bowel disease
Absorption of folate occurs in the jejunum. The total body stores is 5 – 10 mg, which should be sufficient to support 3 – 4 months of folate deprivation.
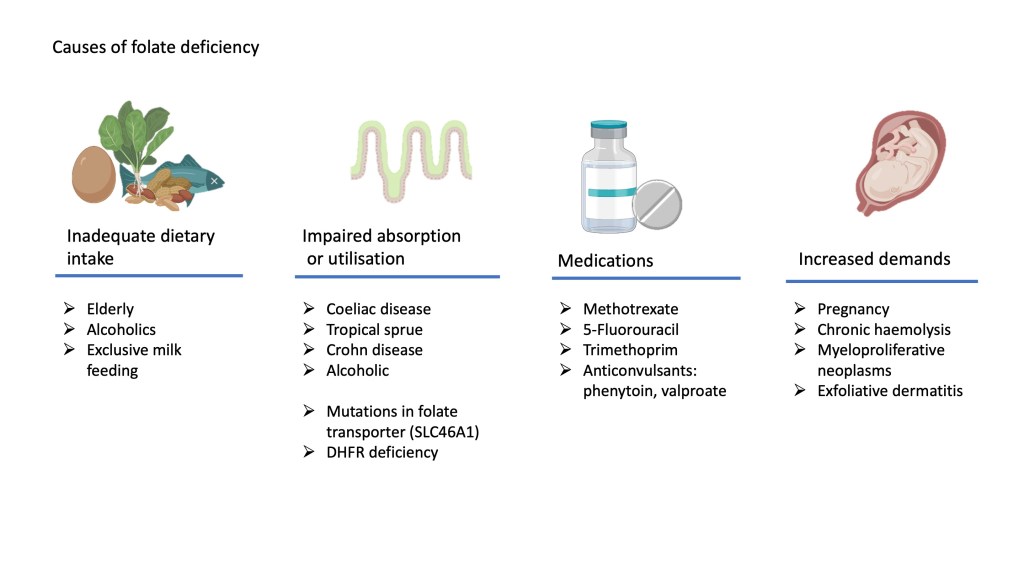
Causes of folate deficiency
The most common cause of folate deficiency is due to inadequate dietary intake, especially in groups that have increased need for folate as mentioned above.
Medications that interfere with purine/pyrimidine metabolism can contribute to folate deficiency. Chemotherapy agents such as methotrexate (MTX) and 5-fluoro-uracil (5-FU) inhibit the action of dihyrofolate reductase (DHFR) and thymidylate synthase respectively. Trimethoprim, an antibiotic also inhibits DHFR. Anticonvulsant drugs such as phenytoin and valproate may also have anti-folate properties.
Clinical features
Apart from general sign and symptoms of anaemia as described in the section on anemia, patients with folate deficiency may show glossitis, characteristically described as beefy red tongue and angular stomatitis. Severe cases may present with anorexia, weight loss and diarrhoea due to its effects on the intestinal mucosa.
Babies born to mothers with folate deficiency have a higher risk of developing neural tube defects (NTD). Folate supplementation in women planning to get pregnant and during pregnancy is therefore very important to prevent this devastating complication in the baby.
Laboratory features
Haematological investigations
The full blood count in folate deficiency will show features of macrocytosis, anisocytosis, moderate neutropenia and thrombocytopenia with hypersegmented neutrophils. These features are common to megaloblastic anaemia due to any cause and is indistinguishable from vitamin B12 deficiency. Reticulocyte count is low or normal unless the patient has been commenced on treatment.
Biochemical investigations
Serum folate would be reduced. Unless the patient has concomitant vitamin B12 deficiency, serum vitamin B12 would be normal.
Serum homocysteine would be high although this test is of low specificity, as vitamin B12 deficiency and several other unrelated conditions may cause an increase in serum homocysteine.
Treatment
The cause of folate deficiency should be identified and treated accordingly. Patients may need to be investigated for underlying malabsorption such as coeliac disease if there is no dietary deficiency. A drug history is also important.
Treatment should be with oral folate for at least three months and may need to be continued indefinitely if the underlying cause cannot be remedied (e.g. chronic haemolysis, thalassaeate mia).
Folate should not be administered alone until vitamin B12 deficiency has been excluded since folate may aggravate or precipitate B12 neuropathy in severely B12 deficient patients. This aspect will be covered in the section on vitamin B12 deficiency.
