Learning outcome
- List the vitamin K dependant factors
- Explain the mechanism underlying vitamin K deficiency and bleeding
- Explain the role of warfarin as an anticoagulant and its action on the vitamin K redox cycle
- Describe the causes, clinical and laboratory features of vitamin K deficiency and warfarin overdose
Vitamin K dependant factors and the vitamin K redox cycle

Among the coagulation factors, FII (prothrombin), FVII, FIX and FX (1972 for short), are considered as vitamin K dependent factors. These factors interact with the phospholipid membrane surface as part of ‘intrinsic tenase’, ‘extrinsic tenase’ and prothrombinase complexes. The interaction between the membrane surface and coagulation factor is facilitated through Ca2+ dependent binding to γ-carboxylglutamic acid residues present on the amino terminal end of the factors.
The γ-carboxylglutamic acid is synthesised by the post-translational modification of glutamic acid residues of factors II, VII, IX and X. This reaction is catalysed by hepatic γ-glutamyl carboxylase that requires reduced vitamin K, oxygen, and carbon dioxide. Therefore, Factors II, VII, X and X are considered as vitamin-K dependant factors since they only function if they are γ-carboxylated in the presence of reduced vitamin K.
The anticoagulant proteins, protein C and protein S are also γ-carboxylated and vitamin-K dependent.
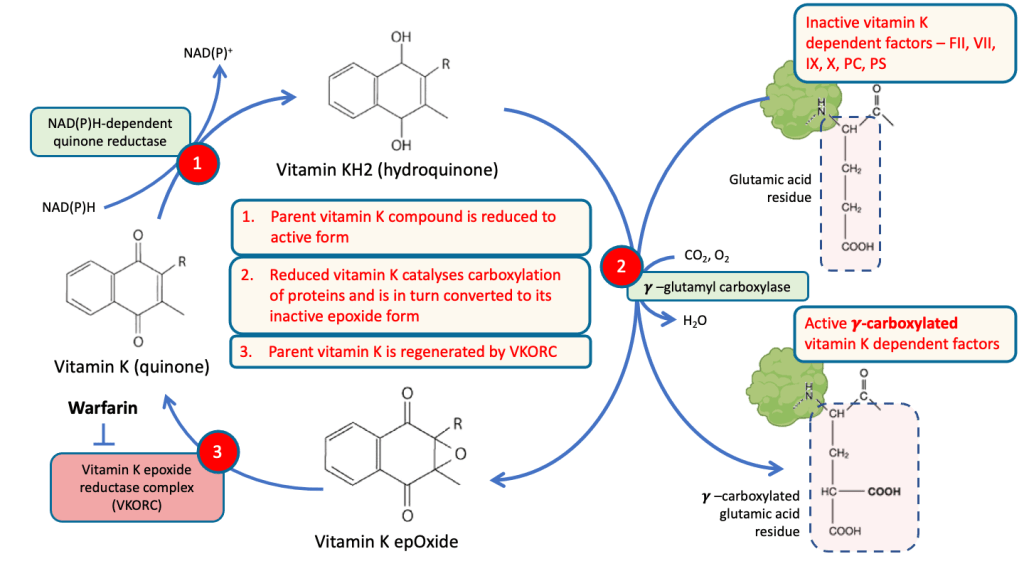
The γ-carboxylation of vitamin K dependent coagulation factors is facilitated by the vitamin K redox cycle in which the parent vitamin K cycles through its reduced and epoxide states. Vitamin K is reduced in the liver by vitamin K reductase to its hydroquinone, vitamin KH2. This then catalyses the carboxylation of the inactive non-carboxylated vitamin K dependent factors via the enzyme γ-glutamyl carboxylase and is converted to its epoxide form.
Vitamin K is thereafter regenerated by the vitamin K epoxide reductase complex (VKORC) to reenter the vitamin K redox cycle.
Risk factors
The source of vitamin K is through;
- Dietary intake. Leafy greens such as spinach, and cauliflower are rich sources of vitamin K.
- Gut microbial synthesis. The chief source of vitamin K is actually synthesis by bacteria in the large intestine. Absence of dietary vitamin K is not particularly deleterious as it can be can be compensated from microbial sources.
- Foetus obtain vitamin K by transplacental transfer. At birth, the neonate has virtually no liver vitamin K reserves. Breast milk is a poor source of vitamin K and the newborn may not have developed gut bacteria to synthesise vitamin K. Newborns therefore are at high risk of vitamin K deficiency.
Vitamin K is a fat-soluble vitamin and both dietary and microbial vitamin K are absorbed into intestinal lymph along with other lipids.
Vitamin K deficiency may be associated with;
- Dietary deficiency is generally rare but can be observed in some vulnerable populations such as those who very ill e.g. cancer patients on chemotherapy, chronic dialysis, malnutrition, alcoholics
- Malabsorption especially when associated with impaired absorption of fats e.g. cystic fibrosis, coeliac disease, chronic pancreatitis, Crohns disease.
- Cholestatic liver disease e.g. bile duct obstruction, primary biliary cirrhosis
- Newborns
- Medications, such as antibiotics, antacids, and anti-epileptics that can interfere with the absorption of vitamin K or decrease production of gut microbial derived vitamin K
Liver disease
All coagulation factors with the exception of von Willebrand factor is synthesised in the liver. von Willebrand factor is synthesised in endothelial cells. FV and FVIII can also be produced by megakaryocytes and endothelial cells, apart from the hepatocytes. Other factors that regulate anti-coagulation (e.g. protein C, protein S, anti-thrombin) as well as fibrinolysis (e.g. plasminogen) is also produced in the liver.
In addition, the liver is responsible for γ-carboxylation of vitamin K dependent coagulation factors as well as facilitating vitamin K absorption from the intestine. Liver failure also leads to a reduced capacity to clear activated coagulation factors and anticoagulants.
Therefore, it is not surprising that PT and APTT are often deranged in liver disease. TT and fibrinogen are not severely effected until late stages when liver function has virtually disappeared.
Warfarin
Warfarin is an anticoagulant that is commonly used to prevent thrombosis in patients at risk, such as those who have venous thromboembolism or atrial fibrillation. It is a vitamin K antagonist that acts by blocking the action of vitamin K epoxide reductase (VKORC), thereby preventing the regeneration of vitamin K. This results in failure of γ-glutamyl carboxylation of vitamin dependant coagulation factors and the accumulation of inactive non-carboxylated forms (PIVKA – proteins induced by vitamin K absence).
Deficiency of functional factors II, VII, IX and X results in disruption of the coagulation process involving both the intrinsic and extrinsic arms. Consequently, both PT and APTT are prolonged. TT is however normal as fibrinogen is not effected by warfarin.
Treatment with warfarin must be tightly monitored to ensure that it is within therapeutic range. International normalised ratio (INR) is a standardised method for reporting the prothrombin time (PT) and is used to monitor warfarin therapy. Above therapeutic INR indicates that the patient is overdosed and is at increased risk of bleeding while below therapeutic INR indicates that the warfarin dose is inadequate and the patient may risk thrombosis.
The therapeutic dose of warfarin may be influenced by many factors that alter vitamin K absorption. Medications that induce or inhibit cytochrome-P (CYP) activity may also alter availability of warfarin as CYP is responsible for metabolism of warfarin.
Clinical features and management
Haemorrhagic disease of the newborn
Newborns with vitamin K deficiency can develop haemorrhagic disease of the newborn, within the first few weeks of life. Babies can present with cephalhaematoma, intracranial bleeding, skin and mucosal bleeds or excessive bleeding from the umbilical stump and vaccination sites. The APTT and PT/INR is prolonged with normal TT.
In Malaysia, all babies are administered prophylactic intramuscular vitamin K to prevent vitamin K deficiency bleeding. In cases of severe life-threatening bleeding, intravenous vitamin K and blood transfusions can be given along with fresh frozen plasma to reduce the bleeding.
Warfarin toxicity
Warfarin levels above therapeutic dose can cause severe bleeding such as intracranial bleeds and gastrointestinal haemorrhage. The PT/INR would be significantly elevated together with prolonged APTT. TT would be normal. Management option of patients who exhibit bleeding secondary to warfarin toxicity would include;
- Discontinue warfarin temporarily
- Administer oral or intravenous vitamin K
- Administer fresh frozen plasma or prothrombin complex concentrates (PCC) which contain factors II, VII, IX
The management options above should take into consideration, the level of PT/INR, severity of the bleeding and patient’s co-morbid conditions as well as his risk for severe bleeding.
Vitamin K deficiency bleeding due to other causes
As described in the section on risk factors, many conditions can predispose to vitamin K deficiency in ill patients. Severe bleeding is not common. However, impaired coagulation secondary to vitamin K deficiency can aggravate bleeding from other sources. Vitamin K administration would reverse the prolonged PT/INR and APTT and reduce bleeding symptoms, if any. Fresh frozen plasma may be administered if there is clinically significant bleeding.
