Mr. Raj is a 26-year-old biomedical-science postgraduate student who notes sudden onset of fatigue, fever, and gum bleeding while brushing his teeth in the last two days. He also reports mild shortness of breath and dizziness.
History
Raj has generally been well and active before this. His symptoms only appeared over the past two days, which he initially attributed to a viral infection, but became increasingly worried after noticing gum bleeding when brushing his teeth that remained persistent since this morning. He also notes pin point red spots over his forearm and bruising over his lower limbs which only appeared today. No epistaxis, haemetemesis or rectal bleeding was reported. He also reported feeling feverish and generally unwell with lethargy and shortness of breath on exertion even when walking short distances.

There was no complaints of abdominal pain, loss of appetite or recent loss of weight. Raj is non-vegetarian and takes a normal Asian and Western diet.
He has been previously well with no significant past medical history. He had a medical check-up done about six months ago when entering his postgraduate programme, when he was informed that he had no medical issues. He is not on any regular medications.
He is a non-smoker, denies drug abuse, is sexually active, partnered and lives together with his female partner in Kuala Lumpur. He gets partial financial support from his parents who own a retail business.
Physical examination
Raj appeared alert with good nutritional status. He appeared short of breath when talking. There was pallor with no evidence of scleral icterus. A few petechial rashes were noted over both forearms and there were large bruises over both shins and knees.
Gum bleeding with with oozing was noted. Dental hygiene was good and there were no oral ulcers or white mucosal patches. No retinal bleeds was visualised.
His weight and height was 64kg and 172cm respectively. Vitals signs were: BP: 130/80mmHg, PR: 92/min, RR: 16/min. He was febrile with temperature of 38oC.
Cardiovascular examination showed normal heart sounds with no murmurs. Breath sounds were normal on lung examination with no crepitations or ronchi. No palpable masses was detected on abdominal examination. The liver and spleen were not palpable. No neurological abnormalities were elicited.
Tasks (Part I) – hypothesis generation
- List three possible diagnosis in order of likelihood (principal diagnosis and differential/other diagnosis).
- For each possible diagnosis listed, provide findings from the history and clinical examinations or patient risk factors that would support your diagnosis.
- For each possible diagnosis listed, provide findings opposing the hypothesis, or findings that were expected but not present or elicited during the clinical examination.
- Based on your reasoning above, decide on the first-line laboratory and imaging tests that you would want to perform in the patient. For each test, state how the results may help you to affirm or disprove your hypothesis.
Investigations (first-line)
Haematology & Clinical Chemistry
| Reference range | Units | ||
| Full blood count | |||
| WBC | 3.8 | 4.0 – 11.0 | 109/L |
| RBC | 2.7 | 3.8 – 4.8 | 1012/L |
| Hb | 72 | 120 – 160 | g/L |
| Hct | 0.23 | 0.37 – 0.47 | |
| MCV | 86 | 77 – 97 | fL |
| MCH | 27 | 27 – 32 | pg |
| MCHC | 318 | 315 – 345 | g/L |
| RDW | 17.2 | 11.5 – 15.0 | % |
| Platelet | 26 | 150 – 400 | 109/L |
| Total white differential counts | |||
| Neutrophils | 1.8 (47%) | 2.0 – 7.5 | 109/L |
| Lymphocytes | 1.7 (45%) | 1.5 – 4.0 | 109/L |
| Monocytes | 0.1 (2%) | 0.2 – 0.8 | 109/L |
| Eosinophils | 0.1 (2%) | 0.04 – 0.4 | 109/L |
| Basophils | 0 | 0.02 – 0.1 | 109/L |
| Metamyelocytes | 1% | ||
| Myelocytes | 1% | ||
| Blasts | 2% | ||
| NRBC | 1/100 WBC | ||
| Serum electrolytes | |||
| Sodium | 138 | 135 – 148 | mmol/L |
| Potassium | 5.2 | 3.5 – 5.5 | mmol/L |
| Chloride | 95 | 95 – 105 | mmol/L |
| Calcium | 2.6 | 2.1 – 2.7 | mmol/L |
| Magnesium | 0.8 | 0.7 – 1.0 | mmol/L |
| Urea | 6.8 | 2.5 – 6.5 | mmol/L |
| Creatinine | 122 | 45 – 120 | mmol/L |
| Coagulation screen | |||
| PT | 21 | 11 – 15 | seconds |
| INR | 2.1 | 0.9 – 1.1 | seconds |
| APTT | 65 | 25 – 35 | seconds |
| TT | 21 | 15 (control) | seconds |
| Fibrinogen | 0.8 | 2 – 4 | g/L |
| D-dimer | Positive | ||
Peripheral Blood Film
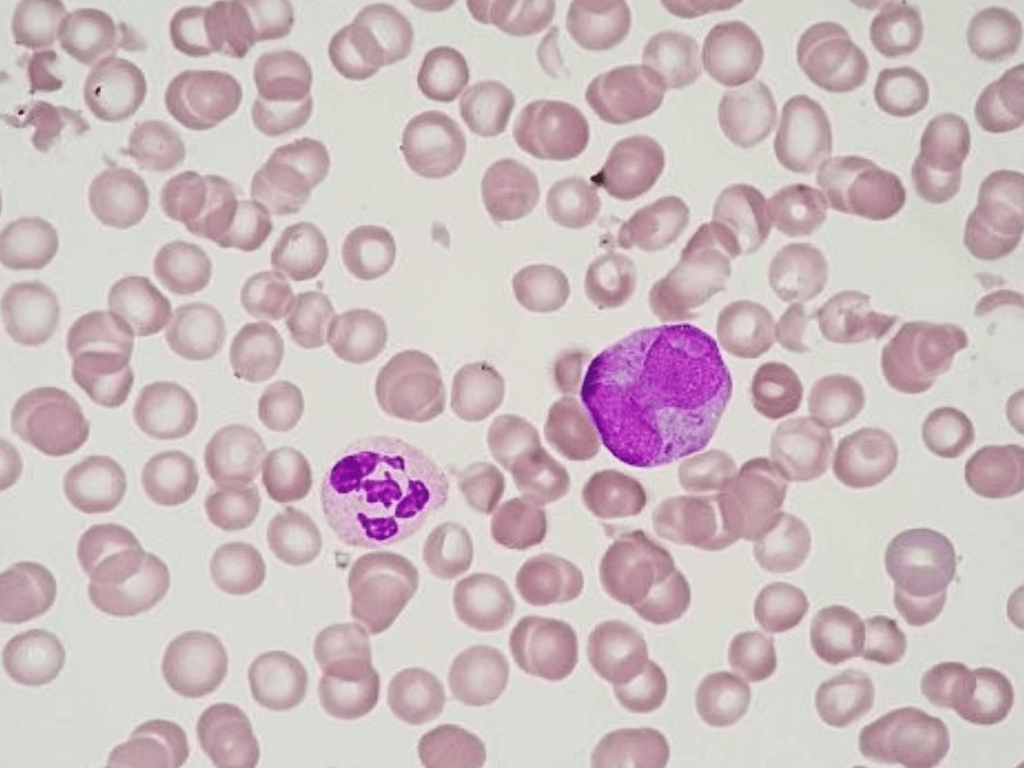
Red cells are reduced in numbers with generally normochromic normocytic cells. Several schistocytes are seen. No significant polychromasia but NRBCs are present.
Platelets and white cells are reduced with neutropenia and left shifted maturation. Occasional blasts with folded nuclei and granular cytoplasm is seen.
Impression: Leucoerythroblastic picture with features suggestive of acute leukaemia. A bone marrow examination would be advised.
Tasks (Part II) – information integration and interpretation
- Refine your diagnosis based on the results of the investigation and reprioritise if necessary
- Formulate the next steps in investigation for confirmation of diagnosis, patient assessment prior to treatment initiation and prognostication
Investigations (additional)
Haematology – bone marrow examination
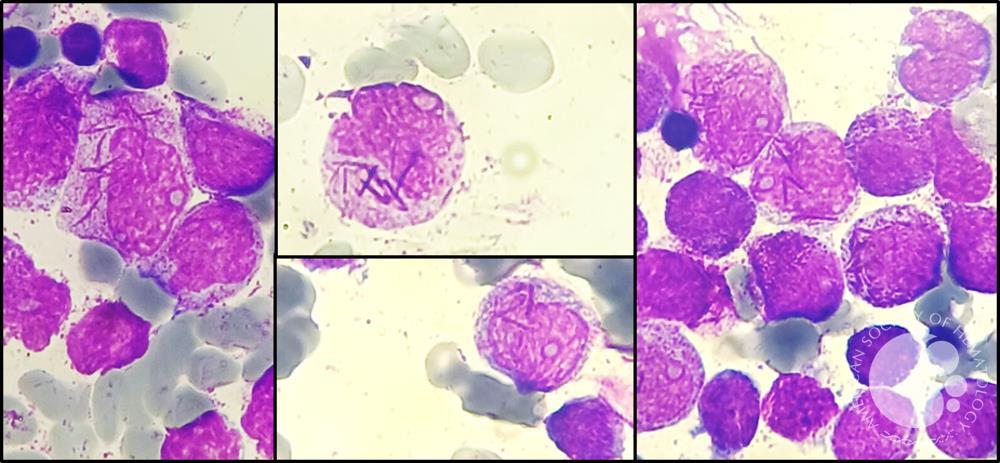
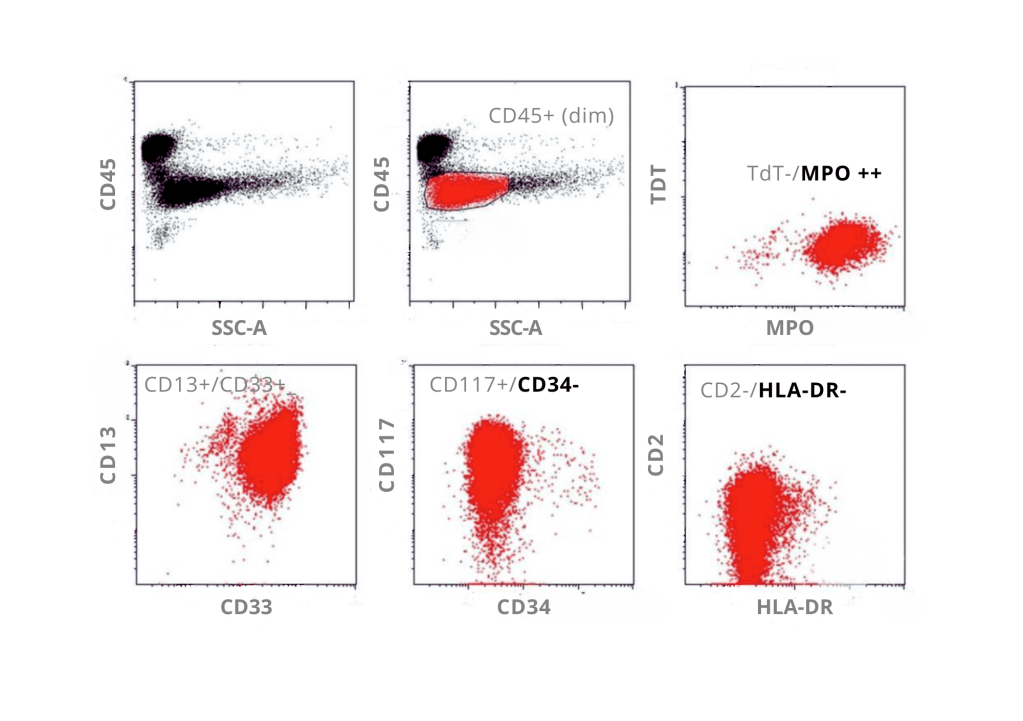
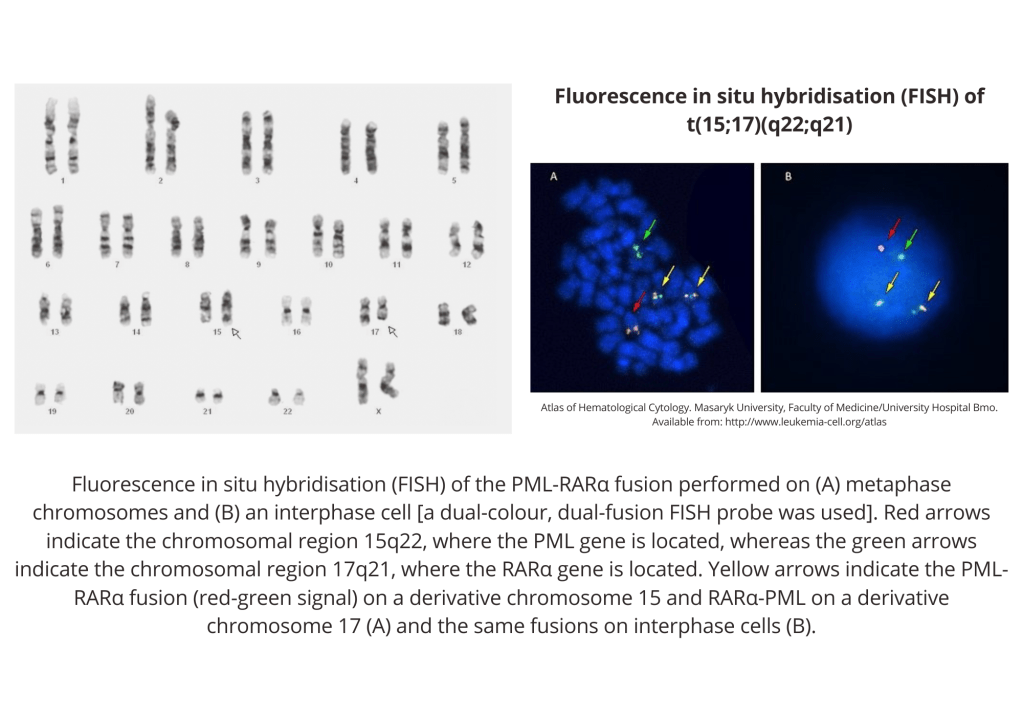
Flow cytometry show cells with absence of HLA-DR and CD34 and expression of CD13, CD33, and CD117; immunophenotypic features are that of acute promyelocytic leukemia.
Tasks (Part III) – mechanistic diagram and management
- Develop a mechanistic diagram outlining the scientific mechanisms behind the major signs, symptoms and laboratory results seen in the patient
- Develop a basic care plan for the patient which should address the physical, mental, and social wellbeing needs of the patient
