
Sean Chiew is a 14-month-old boy. His mother brings him to the Emergency Department because Sean was noted to be limping with a right swollen knee, which seems to be progressively increasing in size over the past couple of hours.
History
The swelling and limp had occurred suddenly. Mrs. Tan, the mother had bathed him about 2 hours earlier and the knee was normal then. He is an active child and had just started to walk by himself although he has had a few falls. The mother did note though that he has had bruising on his body, more commonly then his siblings at the same age, but she attributed this to him being overly active.
Sean is on solids and eating well, with normal growth and development. He was delivered by spontaneous vaginal delivery at term with no complications and has completed all immunisations. There was no history of recent fever or infections, or exposure to any medications.
Sean is the youngest of 3 children (brother is 8 years old and sister is 3 years old). Both parents are of Chinese descent. No history of similar problems in any of her family members or the other siblings was reported. His father, Mr. Chiew is a lawyer while Mrs. Tan is a teacher. They have a full-time maid who helps with the household chores and looks after the children. The family is financially stable.
Physical examination
Sean was alert and responsive. He was crying and holding the right knee in a semi-flexed position. No pallor or jaundice was appreciated. Small bruises of various age were seen over both upper and lower limbs. No retinal haemorrhages were noted.
His weight was 12.5kg with length of 80cm which was above the 50th-percentile. He had a PR of 105/min and temperature of 36.8oC.
Oral examination showed no abnormalities or bleeding. No peripheral lymphadenopathy was noted. Cardiovascular examination showed normal heart sounds with no murmurs. Lungs appeared clear. No palpable masses was detected on abdominal examination. The liver and spleen were not palpable. No neurological abnormalities were elicited.

The right knee was swollen with loss of the knee contours. The overlying skin was warm to touch and tender. Range of movement was limited and was noticeably painful on extension. No muscle wasting was evident and the other joints were normal.
Tasks (Part I) – hypothesis generation
- List three possible diagnosis in order of likelihood (principal diagnosis and differential/other diagnosis).
- For each possible diagnosis listed, provide findings from the history and clinical examinations or patient risk factors that would support your diagnosis.
- For each possible diagnosis listed, provide findings opposing the hypothesis, or findings that were expected but not present or elicited during the clinical examination.
- Based on your reasoning above, decide on the first-line laboratory and imaging tests that you would want to perform in the patient. For each test, state how the results may help you to affirm or disprove your hypothesis.
Investigations (first-line)
Haematology & Clinical Chemistry
| Reference range | Units | ||
| Full blood count | |||
| WBC | 9.4 | 4.0 – 11.0 | 109/L |
| RBC | 3.8 | 3.6 – 5.2 | 1012/L |
| Hb | 105 | 105 – 135 | g/L |
| Hct | 0.29 | 0.32 – 0.44 | |
| MCV | 76 | 70 – 86 | fL |
| MCH | 27 | 21 – 31 | pg |
| MCHC | 281 | 273 – 327 | g/L |
| RDW | 12.6 | 11.5 – 15.0 | % |
| Platelet | 262 | 150 – 400 | 109/L |
| Total white differential counts | |||
| Neutrophils | 1.8 | 2.0 – 6.0 | 109/L |
| Lymphocytes | 6.5 | 5.5 – 8.5 | 109/L |
| Monocytes | 0.7 | 0.7 – 1.5 | 109/L |
| Eosinophils | 0.4 | 0.3 – 0.8 | 109/L |
| Basophils | 0.02 | 0.02 – 0.1 | 109/L |
| Serum electrolytes | |||
| Sodium | 142 | 135 – 148 | mmol/L |
| Potassium | 4.0 | 3.5 – 5.5 | mmol/L |
| Chloride | 99 | 95 – 105 | mmol/L |
| Calcium | 2.6 | 2.1 – 2.7 | mmol/L |
| Magnesium | 0.8 | 0.7 – 1.0 | mmol/L |
| Urea | 2.5 | 1.8 – 6.0 | mmol/L |
| Creatinine | 32 | 23 – 37 | mmol/L |
| Coagulation screen | |||
| PT | 11 | 11 – 15 | seconds |
| INR | 0.9 | 0.9 – 1.1 | |
| APTT | 95 | 25 – 35 | seconds |
| APTT (1:1 Mix) | 35 | 25 – 35 | seconds |
| TT | 15 | 15 (control) | seconds |
Tasks (Part II) – information integration and interpretation
- Refine your diagnosis based on the results of the investigation and reprioritise if necessary
- Formulate the next steps in investigation for confirmation of diagnosis, patient assessment prior to treatment initiation and prognostication
Investigations (additional)
Haematology – coagulation testing
Sean’s results
| Results | Reference range | Unit | |
| FVIII | 1 | 70 – 150 | % |
| FIX | 86 | 70 – 120 | % |
| FXI | 79 | 60 – 120 | % |
| vWF.Ag | 87 | 50 – 200 | % |
| vWF. Activity (CBA) | 75 | 50 – 140 | % |
Mrs. Tan’s results
| Results | Reference range | Unit | |
| FVIII | 68 | 70 – 150 | % |
| FIX | 110 | 70 – 120 | % |
| FXI | 97 | 60 – 120 | % |
| vWF.Ag | 89 | 50 – 200 | % |
| vWF. Activity (CBA) | 80 | 50 – 140 | % |
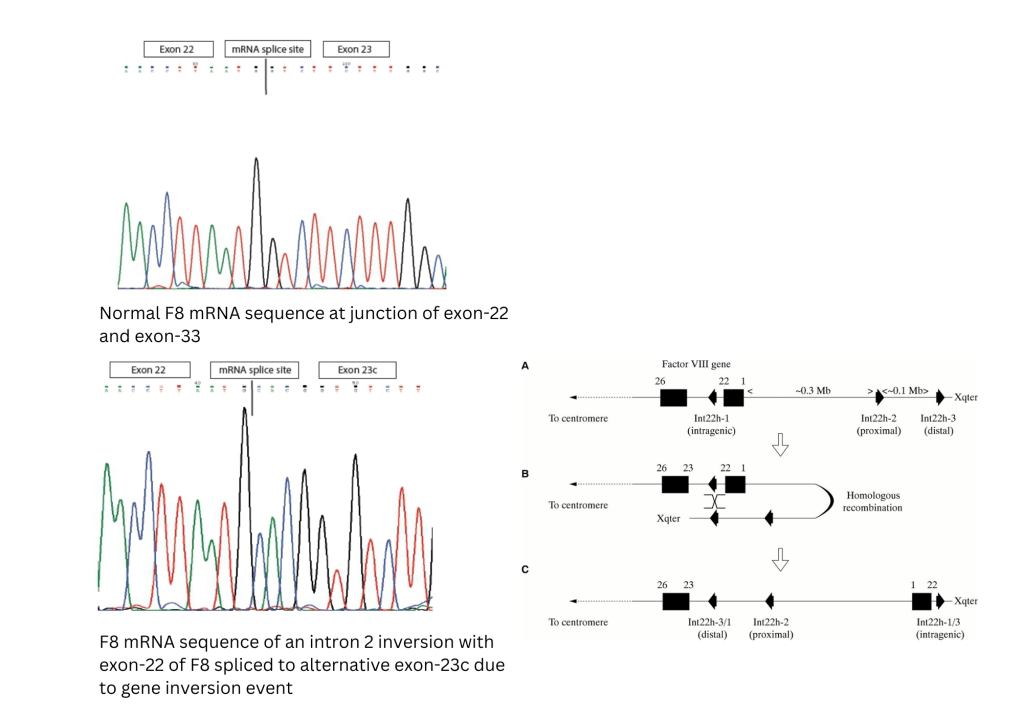
Molecular typing of F8 gene
F8 intron-22 inversion mutation identified in index child (Sean Chiew) and mother (Mrs. Tan)
Molecular Pathology 2002;55:1-18. (2) Hoppers J F, Marx G Μ, Janse van Rensburg W J. Intron 22 inversion real-time polymerase chain reaction detection in haemophilia A families from central South Africa. SAMJ, S. Afr. med. j. 2019; 109( 11 ): 876-879.
Progression
Sean was commenced on recombinant FVIII concentrates to treat the haemarthrosis. The parents were counselled regarding the condition that their son had and education on managing the condition was provided. The parents were also trained on how to administer FVIII concentrates to Sean by intravenous route whenever he had a bleed.

Over the next 6 months, Sean had two additional left knee bleeds which required FVIII infusions. With the third bleed, Mr. Chiew and Mrs. Tan noted that the haemathrosis did not resolve quickly following the FVIII infusion.
Repeat coagulation assessment showed the following results:
| Results | Reference range | Unit | |
| PT | 11 | 11 – 15 | seconds |
| APTT | 110 | 25 – 35 | seconds |
| APTT (1:1 Mix) | 97 | 25 – 35 | seconds |
| FVIII | < 1 | 70 – 150 | % |
| FVIII inhibitor | 3.6 | < 0.5 | Bathesda Unit |
What complication has Sean developed?
Tasks (Part III) – mechanistic diagram and management
- Develop a mechanistic diagram outlining the scientific mechanisms behind the major signs, symptoms and laboratory results seen in the patient
- Develop a basic care plan for the patient which should address the physical, mental, and social wellbeing needs of the patient
